Original Scientific Articles
 Download PDF (29.64 MB)
Download PDF (29.64 MB)
Journal of Structural Heart Disease, February 2016, Volume 2, Issue 1:15-32
DOI: 10.12945/j.jshd.2016.007.14
Atrial Septal Defect: Step-by-Step Catheter Closure
Bharat L. Dalvi1, Shreepal A. Jain2
1 Department of Cardiology, Glenmark Cardiac Center, Mumbai, Maharashtra, India
2 Jaslok Hospital and Medical Research Center, Mumbai, Maharashtra, India
Abstract
Transcatheter device closure of ASD has come a long way since the first experimental closure in dogs by Kings and Mills in 1972. However, unlike earlier devices, the current generation is easier to deploy and retrieve. The secret to a successful procedure includes meticulous planning and execution. It involves comprehensive evaluation from the point of appropriate case selection, detailed pre- and intra-procedural imaging, knowledge of various techniques of device deployment, and anticipating complications and ways to deal with them. In this paper, we describe the step-by-step procedure for transcatheter closure of an atrial septal defect using the Amplatzer Septal Occluder.
Media
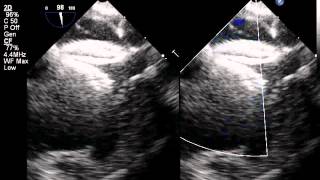
Video 1

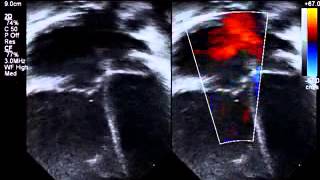
Subcostal bicaval view, documenting adequacy of superior vena caval (SVC) and inferior vena caval (IVC) margins.
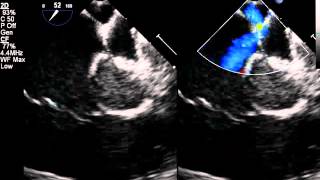
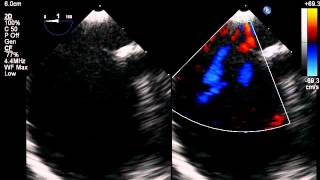
Video 2
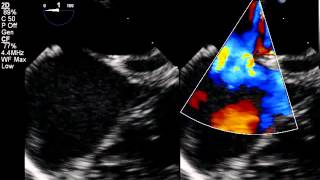
Skewed Apical 4 chamber view with color compare showing the atrio-ventricular (or mitral) margin and the posterior margin.
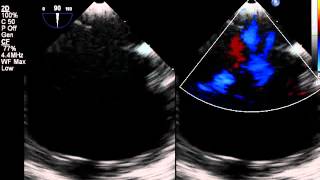
Video 3
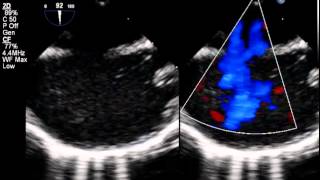
TEE at 0 degrees (4-chamber view), showing the AV valve (or mitral) and the posterior margins.
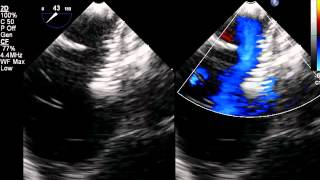
Video 4

TEE at 40 degrees (aortic short axis view), depicting the retroaortic and the posterior margins.
Video 5
TEE at 90 degrees (bicaval view) demonstrates the superior vena caval and inferior vena caval margins.
Video 6

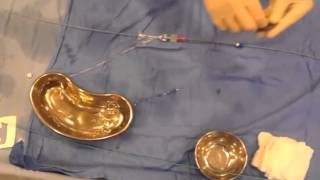
All the components of the delivery system are thoroughly flushed and wiped from outside with heparinized saline solution.
Video 7
It is necessary to load the device after gently messaging it in heparinized saline so as to get rid of the air that might have been trapped in the Dacron patches. It is always a good habit to double check that the device is screwed onto the cable securely.
Video 8

The ASO being slenderized within the loader followed by thorough flushing to get rid of the air within the system.
Video 9

Crossing the defect with a right coronary artery catheter. The catheter tip is positioned in the left superior pulmonary vein (LSPV).
Video 10

A floppy tip Amplatz SuperstiffTM guide wire (Boston Scientific, Marlborough, Massachusetts, USA) being placed in the LSPV.
Video 11

An Amplatzer TorqVueTM 45° delivery sheath (St. Jude, Plymouth, MN, USA) being passed over the Superstiff wire into the mouth of the LSPV.
Video 12

Corresponding TEE loop depicting the delivery sheath being positioned in the LSPV.
Video 13
Delivery sheath being advanced over the dilator into the mouth of LSPV.
Video 14
The delivery sheath positioned in the left atrium just outside the LSPV.
Video 15

Corresponding TEE loop showing the sheath in the left atrium near the opening of the LSPV.
Video 16

Dilator being removed from the sheath to allow back bleed and prevent air embolism.
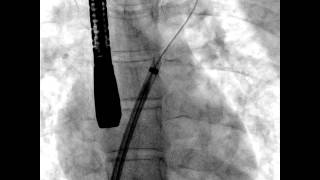
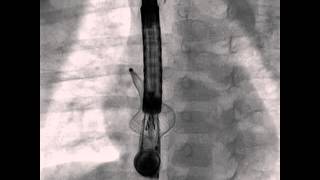
Video 17

Amplatzer septal occluder (ASO) being passed through the delivery sheath.
Video 18
Left atrial disk of the ASO being extruded in the left atrium.
Video 19

Corresponding TEE loop showing left atrial disk in the left atrium.
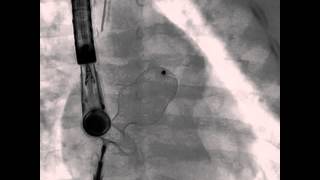
Video 20

The left atrial disk of the ASO being pulled back against the interatrial septum.
Video 21
Corresponding TEE loop depicting the same.
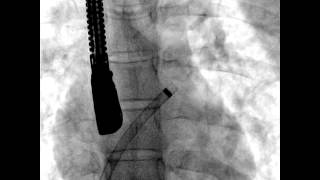
Video 22

Delivery sheath “peeled” back over the loading cable to allow release of the waist and the right atrial disk and deployment of device.
Video 23

Corresponding TEE loop depicting deployment of the ASO across the defect.
Video 24

TEE loops at 0, confirming adequate capture of all margins before releasing the device from the loading cable
Video 25

TEE loops at 45, confirming adequate capture of all margins before releasing the device from the loading cable
Video 26
TEE loops at 90 degrees, confirming adequate capture of all margins before releasing the device from the loading cable
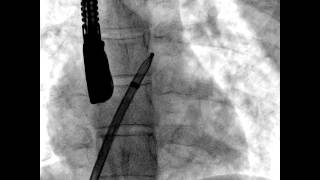
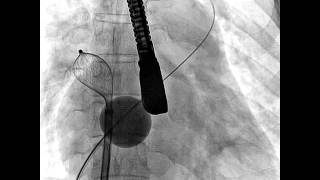
Video 27

Release of the ASO from loading cable in left anterior oblique (LAO) view. Note the well-separated disks of the ASO in LAO view confirming a well-positioned device.
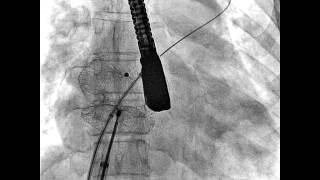
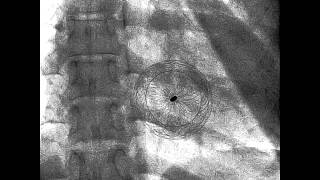
Video 28

Final position of the device in anteroposterior projection; fluroscopic “fingerprinting” of the device.
Video 29
TEE loops depicting a large ASD in a small child. The left atrium is relatively smaller compared to the right atrium.
Video 30

TEE loops depicting a large ASD in a small child. The left atrium is relatively smaller compared to the right atrium.
Video 31
TEE loops depicting a large ASD in a small child. The left atrium is relatively smaller compared to the right atrium.
Video 32
TEE depicting the left atrial disk lying perpendicular to the atrial septum due to inability to accommodate the disk in the left atrium.
Video 33

ASO being deployed via LSPV technique i.e. engaging the LA disk into LSPV. The LA disk disengagement was spontaneous.
Video 34

Corresponding TEE loop depicting the LSPV technique.
Video 35

A contrarian technique of pushing on the cable rather than pulling, to disengage the LA disk.
Video 36
ASO being deployed with the left atrial disk being engaged into the right superior pulmonary vein. Loading cable is pushed to disengage the let atrial disk from the RSPV.
Video 37
ASO being deployed with the left atrial disk engaged in the left atrial appendage. Similar to the previous case, the LA disk has been disengaged from the LA appendage by pushing the loading cable.
Video 38

The delivery sheath has been positioned outside the right superior pulmonary vein instead of LSPV to prevent malalignment of the device disks with the interatrial septum.
Video 39

The ASO device being deployed by this technique.
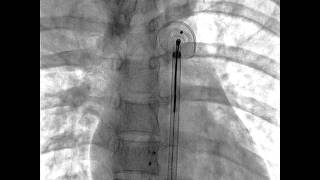
Video 40

An Occlutech balloon is positioned in the right atrium and pushed against the interatrial septum over a Superstiff wire positioned in the LSPV.
Video 41
The balloon is inflated followed by sequential release of the left atrial disk, waist and the right atrial disk.
Video 42

The balloon is gradually deflated to allow deployment of the device across the ASD.
Video 43
The balloon catheter being pulled back into the inferior vena cava before releasing the device.
Video 44
The Superstiff wire now pulled back into the inferior vena cava before releasing the device.
Video 45

Device position confirmed in left anterior oblique view and released.
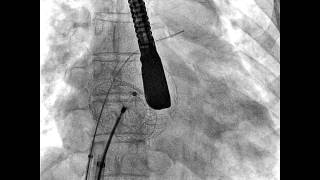
Video 46
ASO being retrieved from the descending thoracic aorta.
Video 47
Absence of leak of contrast agent into the pericardial space after appearing in all the four cardiac chambers.
Cite this article as: Dalvi BL, Jain SA. Atrial Septal Defect: Step-by-Step Catheter Closure. Structural Heart Disease 2016;2(1):15-32. DOI: 10.12945/j.jshd.2016.007.14
All comments will be screened and reviewed before posting. Statements, opinions, and results of studies published in Journal of Structural Heart Disease are those of the authors and do not reflect the policy or position of The Journal and Science International and the Editorial Board and provides no warranty as to their accuracy or reliability. Material is copyrighted and owned by Science International and cannot be used without expressed permission.
Original Scientific Articles
Journal of Structural Heart Disease, February 2016, Volume 2, Issue 1:15-32
DOI: 10.12945/j.jshd.2016.007.14
Atrial Septal Defect: Step-by-Step Catheter Closure
Bharat L. Dalvi1, Shreepal A. Jain2
1 Department of Cardiology, Glenmark Cardiac Center, Mumbai, Maharashtra, India
2 Jaslok Hospital and Medical Research Center, Mumbai, Maharashtra, India
Abstract
Transcatheter device closure of ASD has come a long way since the first experimental closure in dogs by Kings and Mills in 1972. However, unlike earlier devices, the current generation is easier to deploy and retrieve. The secret to a successful procedure includes meticulous planning and execution. It involves comprehensive evaluation from the point of appropriate case selection, detailed pre- and intra-procedural imaging, knowledge of various techniques of device deployment, and anticipating complications and ways to deal with them. In this paper, we describe the step-by-step procedure for transcatheter closure of an atrial septal defect using the Amplatzer Septal Occluder.
Media
Video 1
Video 2
Video 3
Video 4
Video 5
Video 6
Video 7
Video 8
Video 9
Video 10
Video 11
Video 12
Video 13
Video 14
Video 15
Video 16
Video 17
Video 18
Video 19
Video 20
Video 21
Video 22
Video 23
Video 24
Video 25
Video 26
Video 27
Video 28
Video 29
Video 30
Video 31
Video 32
Video 33
Video 34
Video 35
Video 36
Video 37
Video 38
Video 39
Video 40
Video 41
Video 42
Video 43
Video 44
Video 45
Video 46
Video 47
PDF
Mobile-ready Flipbook
Cite this article as: Dalvi BL, Jain SA. Atrial Septal Defect: Step-by-Step Catheter Closure. Structural Heart Disease 2016;2(1):15-32. DOI: 10.12945/j.jshd.2016.007.14
You must be registered and logged in to leave comments.
There have been no comments posted yet
Ask a question (publicly)
Board