Original Scientific Articles
 Download PDF (2.96 MB)
Download PDF (2.96 MB)
Journal of Structural Heart Disease, February 2017, Volume 3, Issue 1:15-27
DOI: 10.12945/j.jshd.2016.005.16
Challenges in Atrial Septal Defect Occlusion
Roie Tal1, Moshe Dotan2, Yitzhack Schwartz1, Avraham Lorber1*
1 Pediatric Cardiology and Adults with Congenital Heart Disease Institute, Rappaport Children’s Hospital, Rambam Health Care Campus, Haifa, Israel
2 Pediatric Cardiology, Ziv Medical Center, Safed, Israel
Abstract
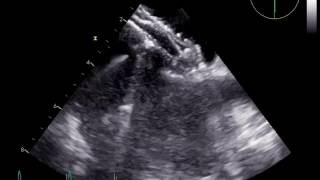
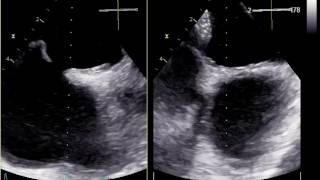
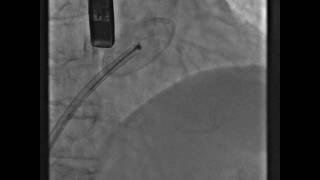
We present 11 cases of percutaneous transcatheter occlusion of atrial septal defects (ASDs) in adults, including multi-fenestrated ASD, balloon-assisted deployment of ASD occlude, dilator-assisted deployment of ASD occlude, "cobra"-shaped disfiguration of the left disc, ASD with deficient aortic rim, pulmonary vein-assisted deployment of ASD occlude, "high" ASD, large Chiari network, double interatrial septum, snaring a runaway occluder, and right ventricular diastolic dysfunction causing cyanosis. Each case is followed by a practical discussion of the special dilemmas, complications, and challenges that may occur during common procedures.
Video 1

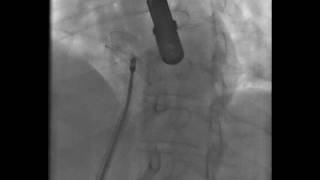
The occluder was malaligned with the defect.
Video 2

The balloon was partially inflated in the defect.
Video 3

The left disc is deployed and held in the left atrium by the balloon
Video 4

Balloon deflation and retrieval while the left disc engaged the left aspect of the interatrial septum.
Video 5
The occluder was released and remained in position.
Video 6

A 32-mm atrial septal defect with reasonable margins.
Video 7

The occluder failed to align appropriately with the interatrial septum.
Video 8

The occluder failed to align appropriately with the interatrial septum.
Video 9

The dilator was introduced to facilitate deployment.
Video 10

The dilator retained the left disc in the left atrium, allowing engagement of the interatrial septum from the right.
Video 11

The dilator retained the left disc in the left atrium, allowing engagement of the interatrial septum from the right.
Video 12

“Cobra”-shape disfiguration of the left disc.
Video 13

Deploying the entire device in the left atrium allowed the device to return to its original shape.
Video 14

Deploying the entire device in the left atrium allowed the device to return to its original shape.
Video 15

Normal deployment and release of the device was possible.
Video 16

Atrial septal defect with deficient aortic rim with an occluder in situ embracing the aortic root.
Video 17

The device was malaligned with the septum.
Video 18

The left disc was partially deployed in upper left pulmonary vein, allowing proper right disc deployment.
Video 19
The device assumed a normal position.
Video 20
Secundum atrial septal defect near the superior vena cava opening into the right atrium.
Video 21

Contrast injection in the superior vena cava confirmed no obstruction to superior vena cava flow.
Video 22

Double interatrial septum.
Video 23
Improper deployment of the entire device in the left atrium.
Video 24
Improper deployment of the entire device in the left atrium.
Video 25

A floating device in the left atrium following its release.
Video 26
A floating device in the left atrium following its release.
Video 27
Video 28

The device was seized and retrieved by biopsy forceps.
Video 29

The device was seized and retrieved by biopsy forceps.
Video 30

Re-deployment of the device.
Video 31

Re-deployment of the device.
Cite this article as: Tal R, Dotan M, Schwartz Y, Lorber A. Challenges in Atrial Septal Defect Occlusion. Structural Heart Disease 2017;3(1):15-27. DOI: 10.12945/j.jshd.2016.005.16
All comments will be screened and reviewed before posting. Statements, opinions, and results of studies published in Journal of Structural Heart Disease are those of the authors and do not reflect the policy or position of The Journal and Science International and the Editorial Board and provides no warranty as to their accuracy or reliability. Material is copyrighted and owned by Science International and cannot be used without expressed permission.
Original Scientific Articles
Journal of Structural Heart Disease, February 2017, Volume 3, Issue 1:15-27
DOI: 10.12945/j.jshd.2016.005.16
Challenges in Atrial Septal Defect Occlusion
Roie Tal1, Moshe Dotan2, Yitzhack Schwartz1, Avraham Lorber1*
1 Pediatric Cardiology and Adults with Congenital Heart Disease Institute, Rappaport Children’s Hospital, Rambam Health Care Campus, Haifa, Israel
2 Pediatric Cardiology, Ziv Medical Center, Safed, Israel
Abstract
We present 11 cases of percutaneous transcatheter occlusion of atrial septal defects (ASDs) in adults, including multi-fenestrated ASD, balloon-assisted deployment of ASD occlude, dilator-assisted deployment of ASD occlude, "cobra"-shaped disfiguration of the left disc, ASD with deficient aortic rim, pulmonary vein-assisted deployment of ASD occlude, "high" ASD, large Chiari network, double interatrial septum, snaring a runaway occluder, and right ventricular diastolic dysfunction causing cyanosis. Each case is followed by a practical discussion of the special dilemmas, complications, and challenges that may occur during common procedures.
Supplemental Media
Video 1
Video 2
Video 3
Video 4
Video 5
Video 6
Video 7
Video 8
Video 9
Video 10
Video 11
Video 12
Video 13
Video 14
Video 15
Video 16
Video 17
Video 18
Video 19
Video 20
Video 21
Video 22
Video 23
Video 24
Video 25
Video 26
Video 27
Video 28
Video 29
Video 30
Video 31
PDF
Mobile-ready Flipbook
Cite this article as: Tal R, Dotan M, Schwartz Y, Lorber A. Challenges in Atrial Septal Defect Occlusion. Structural Heart Disease 2017;3(1):15-27. DOI: 10.12945/j.jshd.2016.005.16
You must be registered and logged in to leave comments.
There have been no comments posted yet
Ask a question (publicly)
Board