Case Reports
 Download PDF (12.38 MB)
Download PDF (12.38 MB)
Journal of Structural Heart Disease, August 2017, Volume 3, Issue 4:119-127
DOI: 10.12945/j.jshd.2017.017.17
Continuous Assessment of a Stented Coronary Artery Using a Pressure Wire During Percutaneous Pulmonary Valve Implantation
Brian A. Boe, MD*, Sharon L. Cheatham, PhD, APRN, ACNP-BC, FSCAI, John P. Cheatham, MD, MSCAI
The Heart Center, Nationwide Children's Hospital, Columbus, Ohio, USA
Abstract
A 52-year-old woman with tetralogy of Fallot status post-complete surgical repair with infundibular resection, pulmonary valvotomy, and patch closure of the ventricular septal defect presented with severe pulmonary regurgitation and depressed right ventricular function. During intended percutaneous pulmonary valve implantation (PPVI), multiple stenotic lesions were discovered in her left anterior descending (LAD) coronary artery, and the procedure was aborted. She underwent treatment of these lesions using drug-eluting stents by our adult interventional colleagues and returned to the congenital catheterization laboratory for PPVI 18 months following her initial procedure. Given the potential risk of crush injury to the coronary arterial stents, the distal LAD artery was continuously monitored during the procedure via a pressure wire with the capability of re-expanding the stent if needed.
Video 1
Three-dimensional rotational angiography performed via a simultaneous power injection in the right ventricular outflow tract and hand injection of the left main coronary artery. The narrowing of the right ventricular outflow tract was located at the native pulmonary valve annulus with the left main coronary artery running immediately behind the right ventricular outflow tract. The stented LAD coursed leftward and posterior to the right ventricular outflow tract.
Video 2

Three-dimensional rotational reconstruction of the right ventricular outflow tract (yellow) and left coronary artery (blue) from dual injection three-dimensional rotational angiography. The left main coronary artery ran posterior to the outflow tract and was superior to the intended valve implantation site at the level of the native pulmonary valve annulus. The LAD coursed leftward and posterior to the right ventricular outflow tract.
Video 3A

Angiography of the right ventricular outflow tract in the anteroposterior (Panel A) and lateral (Panel B) projections. The narrowing of the right ventricular outflow tract occurred at the native pulmonary valve annulus.
Video 3B
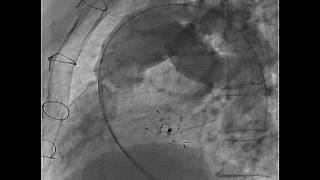
Angiography of the right ventricular outflow tract in the anteroposterior (Panel A) and lateral (Panel B) projections. The narrowing of the right ventricular outflow tract occurred at the native pulmonary valve annulus.
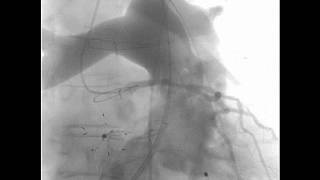
Video 4

Selective left coronary angiography showing the tip of the pressure wire positioned in the LAD distal to the previously placed stents.
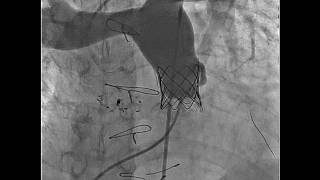
Video 5

Selective left coronary angiography following Melody TPV implantation at steep caudal projections showing no significant coronary arterial narrowing after PPVI. The pressure wire was positioned in the distal LAD.
Video 6
Main pulmonary artery angiography following Melody TPV implantation demonstrating trivial central valvar regurgitation with a catheter through the valve and no paravalvar leak.
Cite this article as: Boe BA, Cheatham SL, Cheatham JP. Continuous Assessment of a Stented Coronary Artery Using a Pressure Wire During Percutaneous Pulmonary Valve Implantation. Structural Heart Disease 2017;3(4):119-127. DOI: 10.12945/j.jshd.2017.017.17
All comments will be screened and reviewed before posting. Statements, opinions, and results of studies published in Journal of Structural Heart Disease are those of the authors and do not reflect the policy or position of The Journal and Science International and the Editorial Board and provides no warranty as to their accuracy or reliability. Material is copyrighted and owned by Science International and cannot be used without expressed permission.
Case Reports
Journal of Structural Heart Disease, August 2017, Volume 3, Issue 4:119-127
DOI: 10.12945/j.jshd.2017.017.17
Continuous Assessment of a Stented Coronary Artery Using a Pressure Wire During Percutaneous Pulmonary Valve Implantation
Brian A. Boe, MD*, Sharon L. Cheatham, PhD, APRN, ACNP-BC, FSCAI, John P. Cheatham, MD, MSCAI
The Heart Center, Nationwide Children's Hospital, Columbus, Ohio, USA
Abstract
A 52-year-old woman with tetralogy of Fallot status post-complete surgical repair with infundibular resection, pulmonary valvotomy, and patch closure of the ventricular septal defect presented with severe pulmonary regurgitation and depressed right ventricular function. During intended percutaneous pulmonary valve implantation (PPVI), multiple stenotic lesions were discovered in her left anterior descending (LAD) coronary artery, and the procedure was aborted. She underwent treatment of these lesions using drug-eluting stents by our adult interventional colleagues and returned to the congenital catheterization laboratory for PPVI 18 months following her initial procedure. Given the potential risk of crush injury to the coronary arterial stents, the distal LAD artery was continuously monitored during the procedure via a pressure wire with the capability of re-expanding the stent if needed.
Supplemental Media
Video 1
Video 2
Video 3A
Video 3B
Video 4
Video 5
Video 6
PDF
Mobile-ready Flipbook
Cite this article as: Boe BA, Cheatham SL, Cheatham JP. Continuous Assessment of a Stented Coronary Artery Using a Pressure Wire During Percutaneous Pulmonary Valve Implantation. Structural Heart Disease 2017;3(4):119-127. DOI: 10.12945/j.jshd.2017.017.17
You must be registered and logged in to leave comments.
There have been no comments posted yet
Ask a question (publicly)
Board